


VenArt Dual Pulse Oximeter
Venous and Arterial Pulse Oximetry
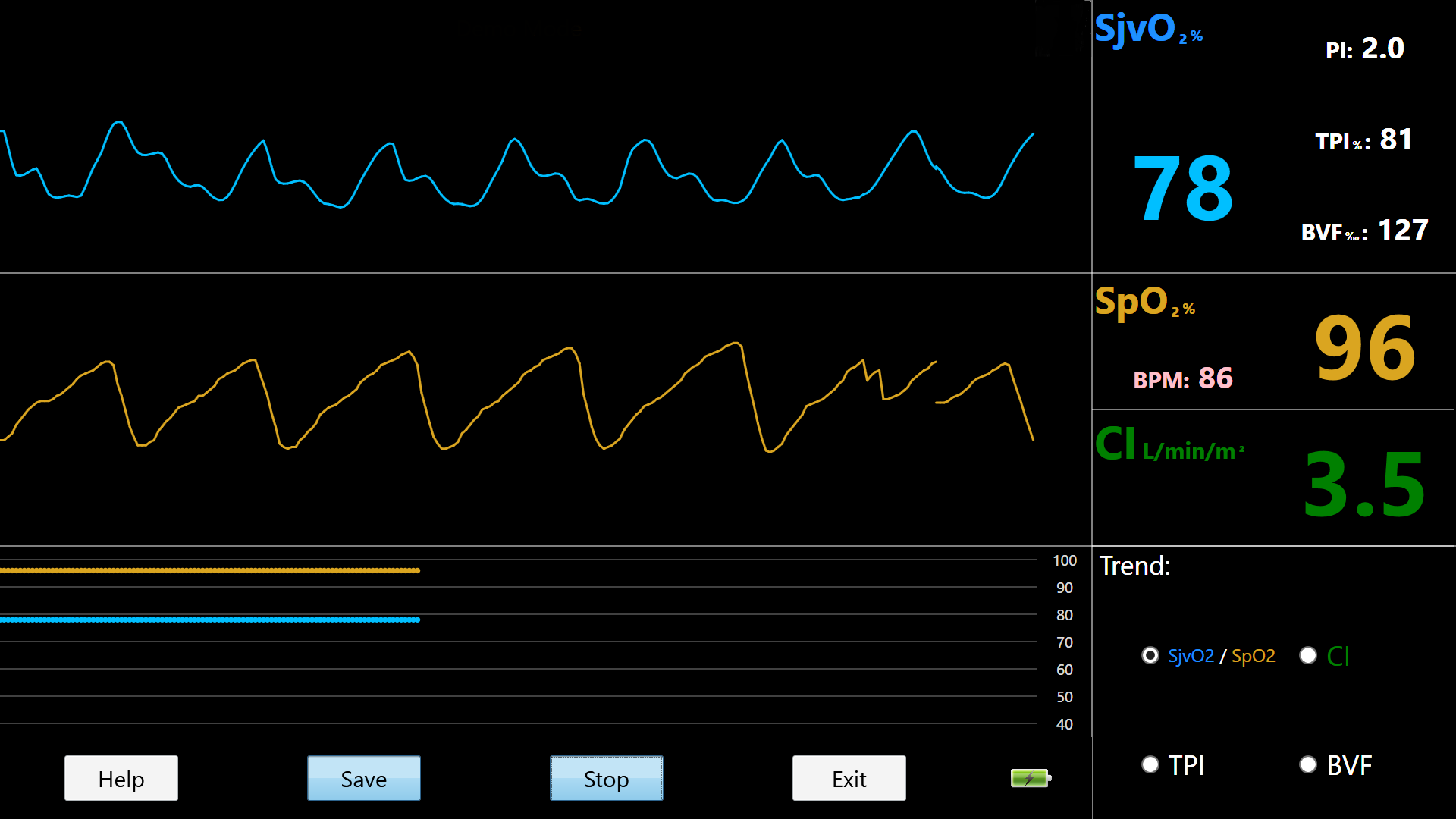
The VenArt Dual Pulse Oximeter is the first-ever non-invasive and continuous assessment system for arterial and venous oximetry with cardiac index


How it works
Traditional pulse oximetry can only measure arterial blood oxygenation. To obtain a full hemodynamic patient picture, venous oxygen saturation must also be assessed. The VenArt Dual Pulse Oximeter extends the utility of the traditional pulse oximeter by allowing for the measurement of both arterial and venous oxygen saturation, at a comparable cost to traditional pulse oximeters. Using these measurements in conjunction with assumed Fick’s determination means that we can provide an additional key parameter: Cardiac Index. This new system can simultaneously assess Cardiac Index and both organ and tissue oxygen consumption and delivery in a continuous manner. The VenArt Dual Pulse Oximeter is the new non-invasive solution for comprehensive total body oxygen supply and utilization monitoring.
Based upon assumed Fick determination, the VenArt Dual Pulse Oximeter is able to non-invasively assess Cardiac Index. Cardiac Index is calculated by dividing the volume of blood pumped by the heart in a minute (Cardiac Output) by the patient’s body surface area (BSA). For more information on how the VenArt Dual Pulse Oximeter calculates Cardiac Index please visit the “Clinical Education” tab.
Performance Features
- Jugular Venous Oxygen Saturation (SjvO 2)
- Pulse Strength Index
- Jugular Venous Pulse Waveform
- Trending SjvO 2
- Arterial Oxygen Saturation (SpO 2)
- Heart Rate (BPM)
- Arterial Waveform
- Trending SpO 2
- Cardiac Index (CI)
- Trending CI
 Health Canada, CE Mark
Health Canada, CE Mark
ISO 13485
Made in Canada
For a PDF version, please download this document.
JVO Education
Physiology and Venous Oxygen Saturation
Venous oxygen saturation (SvO 2) is a measurement used to describe the balance between oxygen delivery and consumption in the brain. SvO 2 has been studied comprehensively, since it has shown to be an improved measurement over the traditional methods (heart rate, blood pressure and central venous pressure). Monitoring jugular venous oxygen saturation (SjvO 2) has been occurring for many decades and has shown to have useful clinical applications for neurosurgical procedures, cardiovascular procedures, head injuries, and sepsis patients.
Monitoring jugular venous oximetry allows clinicians to make more accurate adjustments, in order to improve the patient's wellbeing and will result in better long term outcomes.
Current Method
In the past monitoring involved the use of co-oximetry laboratory analysis and fiber optic technology. Currently the most common device used are fiber optic catheters. Fiber optic catheters are an invasive method. The Mespere VO 100 Jugular Venous Oximetry is a noninvasive continuous jugular venous oxygenation monitoring system, which uses near infrared spectroscopy to measure venous hemodynamics without the need for invasive catheterization.
Interpreting a Change in Venous Oxygen Saturation
The normal range for SjvO 2 is 60-80%, below 60% usually indicates that there is a low oxygen delivery, and above 80% indicates that there is low consumption. When monitoring a patient, clinicians should look for changes of ±5-10% for a period of 5 minutes of longer. If this occurs, that it is an indication of a change in oxygen consumption or demand 1. Jugular desaturation commonly occurs in patients with traumatic brain injury 2, cardiac surgery patients 3, and patients that are comatose.
Accuracy of the Mespere VO 100 Jugular Venous Oximetry Compared to Catheters
Current risks involved with taking a SjvO 2 reading, are catheter placement and maintenance. Catheters are susceptible to conflicting results due to, the rate that the blood is withdrawn, head positioning, and correct tip placement 4. The current precision for commonly used fiber optic catheters, is ±4.41% 5. Contrary to fiber optic catheters, the Mespere VO 100 Jugular Venous Oximetry system is not susceptible to these risks since it is non-invasive, blood is not withdrawn and there is no placement or insertion of a catheter. The accuracy and precision of the Mespere VO 100 Jugular Venous Oximetry is ±2.00%, therefore it is more precise than the current SjvO 2 continuous monitoring methods.
Clinical Applications of Venous Oxygen Saturation
Monitoring jugular venous oxygen saturation (SjvO 2) has been occurring for many decades and has useful clinical application for neurosurgical procedures, cardiovascular procedures, head injuries, and sepsis patients. Continuous monitoring of venous oxygenation, has shown to be a valuable measurement for clinicians. It allows them to monitor the balance between oxygen delivery and consumption. The Mespere VO 100 Jugular Venous Oximetry is a non-invasive continuous jugular venous oxygenation monitoring system that is more accurate, precise, and has far less risks than most commonly used fiber optic catheters.
The Mespere VO 100 Jugular Venous Oximetry is ideal for use in Emergency Departments, Intensive Care Units and in Anesthesia.
References
- Frazier J., Theory and Clinical Application of Continuous Fiberoptic Central Venous Oximetry (ScVO2) Monitoring Edwards Lifesciences
- Roberson CS, Gopinath SP, Goodman JC, et al. SjvO 2 monitoring in head-injured patients. J Neurotrauma 1995;12:891-6
- Croughwell N. Warming during cardiopulmonary bypass. Ann Thorac Surg 1992;53:827-32
- Holly C.G., Matta B.F., Lam A.M., Mayberg T.S., Accuracy of Continuous Jugular Bulb Venous Oximetry during Intracranial Surgery. J. Neurosurgical Anesthesiology 1995:7(3):174-7
- Mahajan A, et al. An Experiment and clinical evaluation of a novel central venous catheter with integrated oximetry for pediatric patients undergoing cardiac surgery. International Anesthesia Research Society 2006; 16:1257-63
CI Education
CI Physiology
Cardiac Output (CO) is an important hemodynamic parameter that explains the volume of blood being pumped out of the heart per minute. Fick’s Principle, states that the volume of the oxygen consumed per unit of time (VO2) is proportional to the difference in oxygen content between arterial (Ca) and venous (Cv) blood. Cardiac Output has the units of L/min.

Cardiac Index (CI) is a hemodynamic parameter that expresses the volume of blood pumped by the heart in a minute (CO) divided by the body surface area (BSA). It is used to evaluate the performance of the heart to the size of the individual. Cardiac Index has the units of L/min/m2.

Current Method
Currently there are numerous methods to measure cardiac output, both invasive and non- invasive, but none are considered the “gold standard”. Invasive methods are more commonly accepted but evidence has proven that they are not necessarily effective in managing therapy, therefore there is a growing need for the development of non-invasive methods. The Mespere Cardiac Index system is a non-invasive and continuous solutions that can help healthcare professionals make an easy and reliable cardiac index assessment.
Interpreting a Change in CI Measurement
Normal range of CI is between 2.6-4.2 L/min/m2. A CI reading outside of this range should be monitored, and appropriate measures should be taken to get the CI back into the normal range.
Mespere LifeSciences Solution for CI
Based upon assumed Fick determination, the Mespere Cardiac Index (CI) system is able to non-invasively assess cardiac index. Because it is very difficult to monitor and measure gas concentrations a common value for VO2 consumption at rest is used, 125mL O 2 per minute per meter of body surface area. It is also a known fact that each gram of hemoglobin can carry 1.34 mL of O 2 and that there is a hemoglobin concentration of 150 grams of hemoglobin per liter of blood. Using these assumptions, the oxygen content can then be calculated with the following formula:

Clinical Applications of Non-Invasive CI
The Mespere Cardiac Index (CI) system is indicated for healthcare professional to measure trending changes in the patient’s body to allow physicians to better understand cardiovascular health. The Mespere Cardiac Index (CI) system should be used by health care professionals as a non-invasive, spot checking and/or continuous assessment tool for physical assessment of cardiac index (CI) of an individual. This is done via an adhesive neck sensor placed over the external jugular vein and a pulse oximeter placed on the patient’s finger. This device is intended for use in hospital and clinical environments.
Mespere Cardiac Index (CI) System
For a PDF version of JVO Education, please download this
document.
For a PDF version of CI Education, please download this
document.
Precision Monitoring
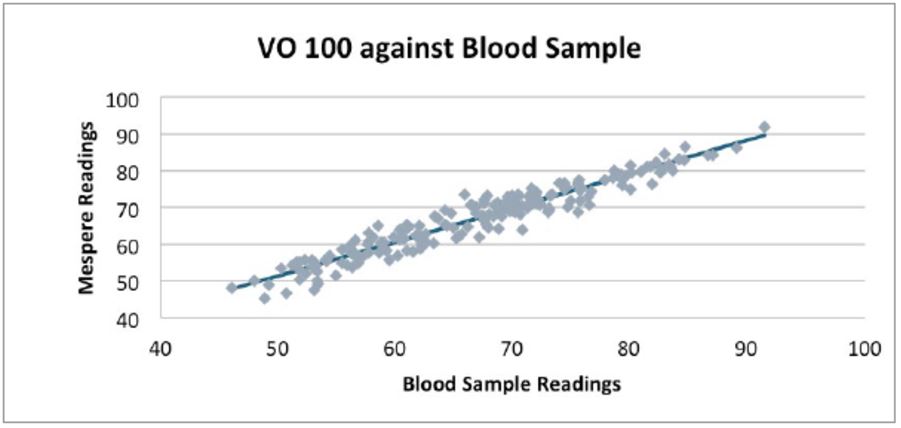
The VO-100 sensor was validated on human subjects through the hypoxia study protocol against blood sample analysis. The Pearson's correlation coefficient is 0.96 and accuracy is =-2.7%
Accuracy of the Mespere VO-100 Jugular Venous Oximetry Compared to Catheters
Current risks involved with taking a SjvO 2 reading, are catheter placement and maintenance. Catheters are susceptible to conflicting results due to, the rate that the blood is withdrawn, head positioning, and correct tip placement 1. The current precision for commonly used fiber optic catheters, is ±4.41% 2. Contrary to fiber optic catheters, the Mespere VO 100 Jugular Venous Oximetry system is not susceptible to these risks since it is non-invasive, blood is not withdrawn and there is no placement or insertion of a catheter. The accuracy and precision of the Mespere VO 100 Jugular Venous Oximetry is ±2.00%, therefore it is more precise than the current SjvO 2 continuous monitoring methods.
Validation
The Venus 2000 CVP are Health Canada approved, CE approved for use in the EU and is pending FDA approval.
References
- Holly C.G., Matta B.F., Lam A.M., Mayberg T.S., Accuracy of Continuous Jugular Bulb Venous Oximetry during Intracranial Surgery. J. Neurosurgical Anesthesiology 1995:7(3):174-7
- Mahajan A, et al. An Experiment and clinical evaluation of a novel central venous catheter with integrated oximetry for pediatric patients undergoing cardiac surgery. International Anesthesia Research Society 2006; 16:1257-63